Mobile Application for Improving the Quality of Life and Elderly
Health Care
Nithikathkul, C.,1* Meenorngwar, C.,1,2 Krates, J.3 and
Kijphati, R.3
1Tropical Health Innovation Research Unit, Faculty of
Medicine, Mahasarakham University, Thailand

2Department of Information Technology, Faculty of
Science and Technology, Valaya Alongkorn Rajabhat University, Thailand
3Bureau of Public Health Research and Innovation
Administration, Division of Academic Affairs,
Department of General Secretary, Ministry of Public Health
*Corresponding Author
Abstract
Imagine a smartphone application that acts as your health
companion, understanding your unique needs and offering guidance
throughout your golden years. This mHealth app aims to improve an
elderly person's health management by analyzing simple physical
tasks to assess key health indicators such as ADL, mood, cognitive
function, mobility, and potential fall risks. It monitors daily
activities to gain insights into overall well-being, identify
potential health risks, and proactively suggest preventive measures
or connect with appropriate healthcare services. Healthcare
services are being offered on the LINE platform through a feature
called "Long-term Care". This feature provides personalized health
advice and recommendations that are tailored to Thai cultural
health beliefs and practices. It also includes interactive
communication to ensure better understanding. To analyze this
feature, a healthcare dataset consisting of 913 samples has been
collected from both Ubon Ratcha Thani and Sisaket provinces. This
dataset will be used with machine learning algorithms. It analyzes
and presents the principal component analysis (PCA) approach of
activities of daily living (ADL), highlighting important features
for AI models. It also allows users to share their health data and
progress with family members or caregivers, enabling informed
decision-making and collaborative care. This can help develop
intervention services for the community. Finally, the team has
successfully developed a mobile health (mHealth) application using
Principal Component Analysis (PCA) to gain data-driven insights. In
the future, they plan to use the identified features to create
personalized intervention protocols for caregivers, which will
improve support for elderly individuals in their Activities of
Daily Living (ADLs). The app integrates with the LINE platform to
encourage community engagement and empower both caregivers and
healthcare providers to provide comprehensive care.
Keywords: DL, Long-Term Care, mHealth, Rajabhat Dataset,
Stress
1. Introduction
Long-term care (LTC) refers to a broad spectrum of services and support
provided to individuals who require assistance with daily living
activities due to chronic illness, disability, or age-related
limitations. These services can be provided in various settings, such
as in-home assistance with daily tasks like bathing, dressing, meal
preparation, and medication management. Assisted living facilities
offer housing and on-site support services for individuals who need
help with daily living but want to maintain their independence.
Additionally, nursing homes provide skilled nursing care and
comprehensive medical services for individuals with complex medical
needs.
Technology applications can play a crucial role in supporting family
caregivers by facilitating access to relevant information, community
resources, and formal and informal services. Monitoring technologies
are particularly useful for caregivers who need to keep an eye on their
loved ones' status or activities while they are away at work or a
remote location. Additionally, telemedicine applications can help care
providers monitor patients' health and deliver healthcare services
effectively [1]. Since LINE has a massive user base in Thailand, it is
easily accessible to both residents and caregivers. The platform
provides Thai language support and eliminates language barriers for
users.
Features such as photos, videos, and voice messages can enhance
communication and provide richer data for ADL monitoring. One crucial
benefit is the "Group chats" feature that facilitates communication
between caregivers, family members, and healthcare professionals
involved in a resident's care. Additionally, LINE's user-friendly
interface makes it easy for both residents and caregivers to navigate,
promoting adoption and reducing training needs. Caregivers can use LINE
groups to record and share daily observations about residents'
activities of daily living (ADLs) through text, photos, or videos. These
observations could include tasks like bathing, dressing, eating,
toileting, and mobility. Caregivers can also share their observations
about residents' mood, sleep patterns, or behavioral changes, which can
help detect potential issues early on. This is suitable for developing
an ADL LINE-based monitoring system that is imperative to have the
cooperation of care facilities, technology providers, and the Thai
community. However, it is crucial to consider local cultural norms and
address potential obstacles to ensure that the implementation is
successful and responsible. This leads to earlier detection, improved
interventions, and better health outcomes for individuals in long-term
care facilities compared to traditional methods.
Collecting real-time ADL data detect functional decline early and
provide personalized interventions, leading to more accurate care plans
and efficient allocation of resources. It increases screening rates for
mental health support, prevents the worsening of symptoms, and gains a
deeper understanding of the relationship between ADL, stress, and
others for necessary treatment adjustments. The support feedback has
led to the development of experiments that integrate protocol
functionality within this mobile application, allowing for remote
consultations with doctors or specialists and improving access to
healthcare. This study aims to develop a mobile healthcare (mHealth)
application called "Long-Term Care" for measuring healthcare metrics
for elderly individuals in the local Thai community. The application
integrates the popular LINE platform with ADL (Activities of Daily
Living) monitoring in long-term care facilities in Thailand to offer
numerous benefits.
For our research, we have developed the "Long-term Care" mobile
application on the popular LINE platform, with the aim of
revolutionizing healthcare management for the elderly in Thailand. This
innovative mHealth app monitors and analyzes daily activities to assess
key health indicators such as ADL, mood, cognitive function, mobility,
and fall risk (Figure 1). It provides personalized health advice
tailored to Thai cultural beliefs and practices, fosters interactive
communication for better understanding, and enables seamless sharing of
health data with family members and caregivers.
2. Literature Review
2.1 How to Develop Long-Term Care Applications?
Technology has significantly improved the quality of life and care for
individuals receiving long-term care. For instance, wearable devices
and sensors can track vital signs, medication adherence, and activity
levels, enabling healthcare providers to monitor patients remotely and
offer virtual consultations. In Japan, they are developing an effective
model to predict an individual's future long-term care demand using
previous healthcare insurance claims data [2].
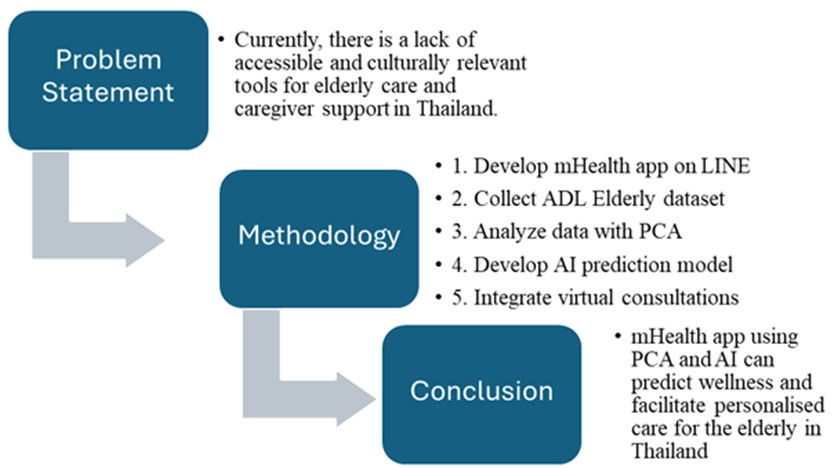
Figure 1: Conceptual design for LTH mHealth app
research
This model uses three learning algorithms with medical and long-term
care insurance claims and enrollment records. Some health apps view
medication as just one part of a larger strategy that includes other
interventions and lifestyle changes to improve patient outcomes. The
first systematic review of eHealth interventions for carers' wellbeing
aims to provide a comprehensive analysis. The review identified 78
studies, which included 62 distinct interventions that aimed to improve
carers' knowledge, self-efficacy, caregiving appraisal, and reduce
health concerns. The studies revealed that dementia was the most
researched area, accounting for 40% of all studies [3]. For example,
the Transitional Care Assessment Tool in Long-Term Care (TCAT-LTC) is
developed which consists of 2 themes, 12 categories and 63 items.
Themes include organizational and financial aspects. Organizational
aspects include categories such as communication, transfer of
information, availability and coordination of resources, training and
education of staff, education/support of the patient/informal caregiver,
involvement of the patient/informal caregiver, telemedicine and eHealth,
and social care. Financial aspects include primary care, hospital, and
long-term care categories [4].
In the realm of mobile application development, a total of 328 apps
were categorized. Out of these, 175 were developed for Android and 153
for iOS. The majority of these apps, 73% (11 out of 15), were developed
by the software industry. In contrast, only 15% (3 out of 20) were
co-developed by healthcare professionals. The remaining 2.1% (7 out of
328) were developed by academia [5]. Gamified apps and interactive
platforms offer personalized exercises for cognitive stimulation and
physical rehabilitation. These integrate information for coordinated
care plans and progress tracking. Privacy and data security compliance
are important. In Spain, it involves a combination of a smartphone
application, an activity tracker wristband, and brief counseling, which
is being compared to a group receiving only brief counseling. The goal
is to evaluate the impact of the intervention on weight loss, body
composition, physical activity, and caloric intake among Spanish
sedentary adults who are overweight or obese [6].
Effective long-term care applications require collaboration between
technology developers, healthcare professionals, caregivers, and
patients. A study in Singapore used classification and regression tree
analysis to find out why some patients and their caregivers didn't take
up referred services [7]. Understanding the needs of those impacted by
long-term care and leveraging technology thoughtfully creates impactful
solutions that improve the quality of life for all involved. Four AI
features - Recommendation, Conversational Agent, Recognition, and
Prediction - are commonly used in seven health domains, including
fitness, mental health, meditation and sleep, nutrition and diet, etc.
[8]. For this study begins by establishing video conferencing
platforms, such as Zoom, to connect patients from Ubon Ratchathani and
Sisaket provinces with healthcare providers. This reduces social
isolation and improves mental well-being. Then, it is being built on
the LINE platform, which is cost-effective and offers benefits and also
be used to monitor health and assess the effectiveness of mobile health
intervention.
This research utilizes the wide user base of the LINE platform in
Thailand, as well as its support for the Thai language and interactive
capabilities, to develop a culturally relevant mHealth app that is
easily accessible (Figure 2). The app can track activities of daily
living (ADLs) and gather real-time data, enabling early identification
of declines in functionality, customized interventions, and better
health results.
2.2 Developing the Application to Support LTC?
The mobile Smart Care System (mSCS) conducted a study to evaluate the
acceptance and usability of a mobile technology with focus groups.
Participants reported that the application supported care coordination
and communication with staff, and showed high technology acceptance
among family caregivers in a long-term care setting. Facilitating
conditions influenced acceptance, which should be optimized for
technology uptake [13]. The health care sector has adopted digital
technology to enhance patient care and clinical support, including the
use of medical knowledge resources and monitoring quality care [14].
LINE is a widely used platform in Southeast Asia, which makes it easily
accessible to a large population who may require long-term care
support. As users are already familiar with the platform's interface
and features, they can easily adopt and learn how to use it. For
instance, LINE groups are useful for patients, family members,
caregivers, and healthcare providers to communicate and coordinate with
each other. They can share updates, schedule appointments, and discuss
care plans together in a streamlined manner. It's important to note that
while the LINE app can provide some long-term care support, it may not
be a viable option for everyone. Its usage isn't as widespread as other
apps, potentially leaving out certain segments of the population.
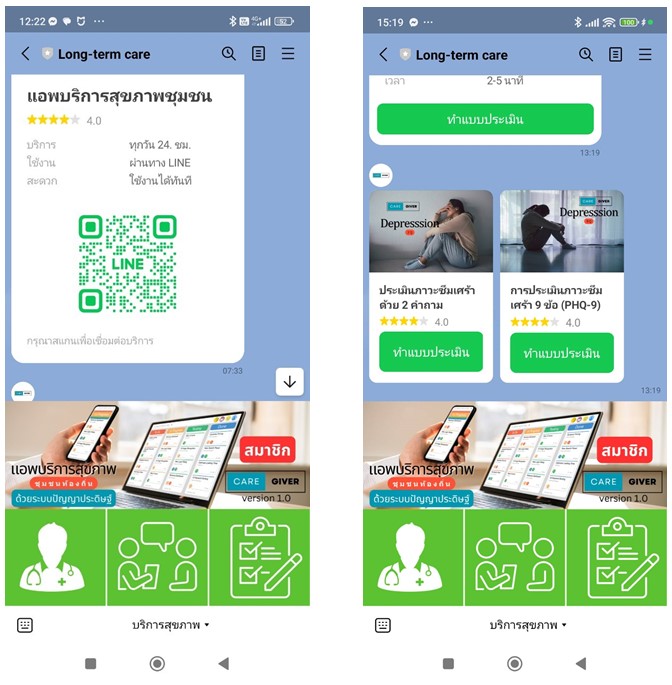
Figure 2: "Long-term care" mHealth prototype
Additionally, digital literacy and device access must be considered,
and the app may not have all the necessary features to provide
comprehensive support. Therefore, integration with other specialized
healthcare platforms and tools may be required. c, especially for those
in rural areas or with limited connectivity, as they may not be able to
fully benefit from the services. We plan to use the mHealth LINE
application to gather data on the elderly and utilize Artificial
Intelligence (AI) to identify suitable Machine Learning algorithms for
predicting the ADL group in specific areas. However, it's important to
note that previous studies have applied AI methods to identify
appropriate datasets, yielding different results, as indicated in Table
1.
A long-term care developer recognizes the potential benefits of using
LINE for communication, information sharing, and social engagement.
However, it is crucial to address privacy concerns, ensure
accessibility and digital inclusion, and consider integrating other
healthcare tools for comprehensive support. This study has developed a
LINE application that can serve as a centralized hub for remotely
monitoring vital signs, medication adherence, and overall well-being.
The application includes health self-assessments such as the ADL,
stress, loneliness scales, and others. It also shares educational
materials, health tips, and information about local resources for
long-term care services and support. Therefore, it works as an open
space to connect with others in similar situations, which can improve
mental well-being and quality of life. This mHealth
application is accessible and user-friendly for individuals with
varying abilities and technology experience. It is crucial for the
application to integrate with existing healthcare systems and platforms
to ensure seamless information flow and care coordination.
2.3 Caregiver with LTC for Elderly Person Services
The pandemic has highlighted the importance of local healthcare for
communities to access services easily. Specifically, long-term care
services for the elderly are crucial to provide a range of assistance
and support for older adults to live safely and comfortably as they
age. In Taiwan, the study assessed variables for caregivers such as
health, education level, job, income, and caregiving period. For care
recipients, factors such as age, education level, living situation, and
dependency level were assessed. Self-rated health was used to measure
the health of both caregivers and care recipients [15].
Home nursing care was linked with better health for caregivers aged 65
or older, but not for those under 65. Caregiver employment, lower
caregiving costs, and higher care recipient health improved the health
of older caregivers. Daughters-in-law involvement and care recipient
health were positively related to the health of younger caregivers. ICT
was utilized to connect various groups including residents' families,
hospitals, specialists, and general practitioners in the long-term care
facilities [16].
Smartphone apps were created for both socializing and telemedicine.
However, there was a lack of peer-to-peer social interaction among the
elderly. As a result, this study aims to categorize LTC services in
different settings such as at home, adult day care centers, assisted
living facilities, or nursing homes based on their significance.
2.3.1 Essential services
The services mentioned below are crucial for meeting basic needs and
maintaining safety. Personal care includes assistance with daily living
activities like bathing, dressing, toileting, eating, and medication
management. [17] Caregivers can help with errands, doctor appointments,
and social outings, while also ensuring access to nutritious meals,
particularly for those with dietary restrictions or difficulty cooking.
They also help with housekeeping, laundry, and shopping to maintain a
clean and comfortable living environment and check in regularly to
ensure the elderly person's well-being and address any immediate
concerns.
Table 1: A comparison table summarizing previous
research
|
Study
|
Dataset
|
Methodology
|
Results
|
|
Development and validation of a prediction model
for cognitive impairment among disabled older adults
[9].
|
Chinese Longitudinal Healthy Longevity Survey
(CLHLS), eighth wave (2017-2018), seventh wave
(2014), and sixth wave (2011).
|
LASSO regression for variable selection, logistic
regression (LR), support vector machine (SVM),
random forest (RF), and XGBoost for model
development
|
LR exhibited the best predictive performance with
an area under the curve (AUC) of 0.875. A nomogram
based on LR using five predictors (age, ADL
score, IADL score, HI, and VI) demonstrated good
discrimination in internal (AUC = 0.871) and
external (AUC = 0.825 and 0.863) validation sets.
|
|
Development and evaluation of a machine learning
algorithm to identify functional impairment using
electronic health record (EHR) data[10].
|
EHR data from 6484 patients
|
Unsupervised learning (K-means and t-SNE) for
patient classification, supervised learning (Extreme
Gradient Boosting) to predict functional status
states.
|
High accuracy in predicting functional status
states (AUROC 0.92, 0.89, and 0.87 for normal
function, mild/moderate impairment, and severe
impairment, respectively). Age, falls,
hospitalization, home health use, labs,
comorbidities, and social determinants of health
were key predictors.
|
|
Prospective cohort study of internal medicine
wards in a tertiary care hospital in China to
develop a machine learning model that predicts
delirium risk in geriatric internal medicine
inpatients [11].
|
40 hospital admissions with a median (IQR) age of
84 (79-87) years, 527 (71.2%) were men, and 101
(13.6%) with delirium.
|
Decision tree model trained on 70% of the data
with five-fold cross-validation, under-sampling to
address class imbalance, and evaluation on the
remaining 30%.
|
The model achieved an AUC of 0.950 and F1 score
of 0.810 on the test set, with 93.3% sensitivity,
94.3% specificity, 71.8% positive predictive
value, 98.9% negative predictive value, and 94.1%
accuracy.
|
|
A two-step hybrid machine learning model to
explore the onset of depression in home-based older
adults [12].
|
Depression data (collected in 2011, 2013, 2015,
and 2018) of home-based older Chinese (n = 2,548)
recruited in the China Health and Retirement
Longitudinal Study
|
Step 1: Long short-term memory network (LSTM) to
identify risk factors in 2015 using the first two
waves of data. Step 2: Three ML classification
algorithms (gradient boosting decision tree,
support vector machine, and random forest) evaluated
with 10-fold cross-validation and AUROC metric to
estimate depression outcome.
|
Time-varying predictors of depression
successfully identified by LSTM (mean squared error
= 0.8). Mean AUCs of the three predictive models
ranged from 0.703 to 0.749. Top five important
variables: self-reported health status, cognition,
sleep time, self-reported memory, and ADL
disorder.
|
2.3.2 Supportive services
These services focus on enhancing the quality of life, promoting
independence, and addressing specific needs. Caregivers provide
opportunities for conversations, socialization, and activities to
combat loneliness and isolation. They engage in various activities such
as brain games, exercise programs, and creative pursuits to maintain
cognitive function and physical health. Additionally, they offer
counseling, support groups, and access to mental health professionals to
address anxiety, depression, or any other mental health concerns. In
Thailand, elderly citizens are often provided with social care
assistance. Caregivers help with tasks such as managing finances,
navigating benefit programs, and making legal decisions related to
aging. As Thailand is a Buddhist country, many individuals in the
community connect with religious or spiritual communities and practices
to address spiritual needs and find comfort.
2.3.3 Advanced services
These are specialized services that cater to individuals with more
complex medical or cognitive needs. Caregivers who are trained nurses
provide medical care such as wound care, medication administration, and
pain management. Physical, occupational, and speech therapy are also
provided to help regain or maintain functional abilities after illness
or injury. Palliative care and support are also provided for terminally
ill individuals and their families.
2.4 Mobile Application for Caregivers
Developing an application for caregivers to assist the elderly with
long-term care services is a wonderful initiative. It has the potential
to significantly improve the lives of both caregivers and those they
care for. For example, a mobile application was used to assess the
effect of an electronic medical record-integrated mobile app for
personalized diabetes self-care. The focus was on the self-monitoring
of blood glucose and lifestyle modifications on glycemic control in
patients with type 2 diabetes mellitus [18].
This idea is addressing a critical need because there is a growing
demand for innovative tools and support systems for caregivers,
especially with the increasing elderly population. The application
utilizes LINE's accessibility and familiarity to reach caregivers
effectively and offer valuable functionalities. It provides resources,
education, and connections to ease the burden of caregivers and improve
the quality of care by assisting with tasks such as medication
reminders, appointments, and access to information (Figure 3).
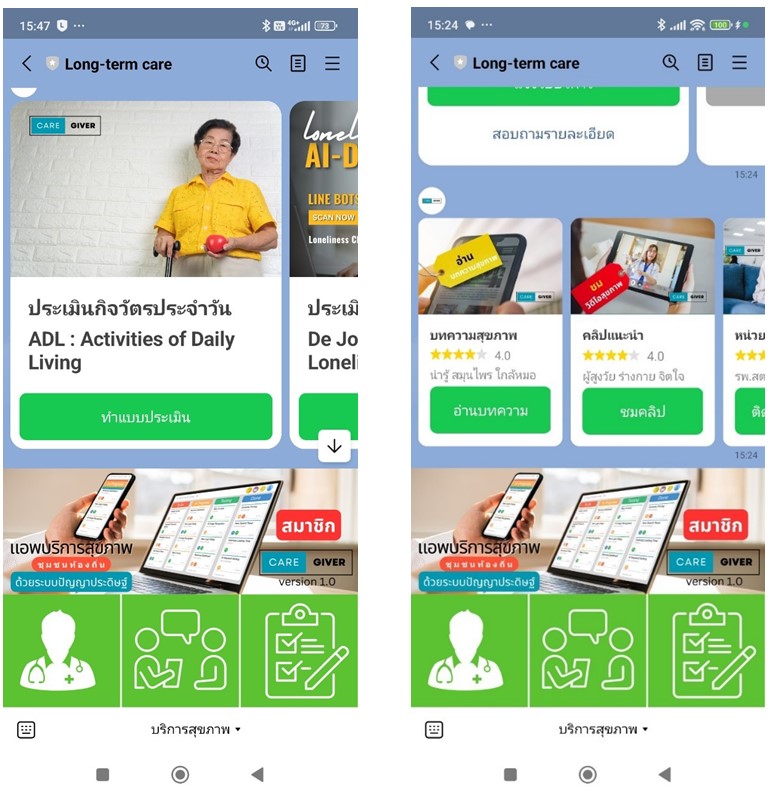
Figure 3: Self-Assessment and Services in mHealth
"long-term" care applications
The application also promotes elderly independence and well-being. In
essence, this application serves as a healthcare notebook for community
members to conveniently collect their health-related activities and
information. iREST is an mHealth example that aims to develop and
assess the usability of a Just in Time Adaptive Intervention
application platform. [19] It was highly usable and easily implemented
across different smartphone platforms. This information can be easily
accessed by doctors or healthcare units to track progress, identify
potential problems, and monitor the completion of behavior-related
tasks.
The ideal caregiver application should prioritizes functions that
address everyday challenges caregivers face, such as scheduling,
coordinating care plans, and accessing relevant resources. The
interaction design of the application should priorities
user-friendliness and accessibility, making it intuitive and easy to
navigate for caregivers of all ages and tech literacy. For example, the
application should feature large fonts for accessibility and connect
with local healthcare providers, community organisations, and delivery
services to provide comprehensive support. Importantly, data security
measures should be in place to protect user information and ensure
adherence to relevant data privacy regulations. It is also important to
provide training for both caregiver associations and senior centers to
promote adoption and offer training workshops for effective app
utilization.
2.4.1 Potential LTC mobile application features
There is a study on technology acceptance to compare mHealth research
treatment with models, identify gaps, and clarify acceptance process
[20]. In developing as a mobile application, it based on the [20]. In developing as a mobile application, it based on the concepts
ement, scheduling and organizing daily routines, medication
schedules, and appointments as tools to connect with family members,
healthcare providers, and other caregivers through calls, video chat,
and messaging platforms. There are various support applications
such as Google Meet, Zoom, Microsoft Teams, or LINE that allow
caregivers and the community to work together by using features such as
emergency alerts and location sharing for immediate assistance and
peace of mind. These applications also provide accessibility to local
services, support groups, and educational materials on elder care. With
the help of mobile devices, caregivers can monitor the progress of
care, medication adherence, and overall well-being of the elderly,
which helps them in making informed decisions (Figure 4).
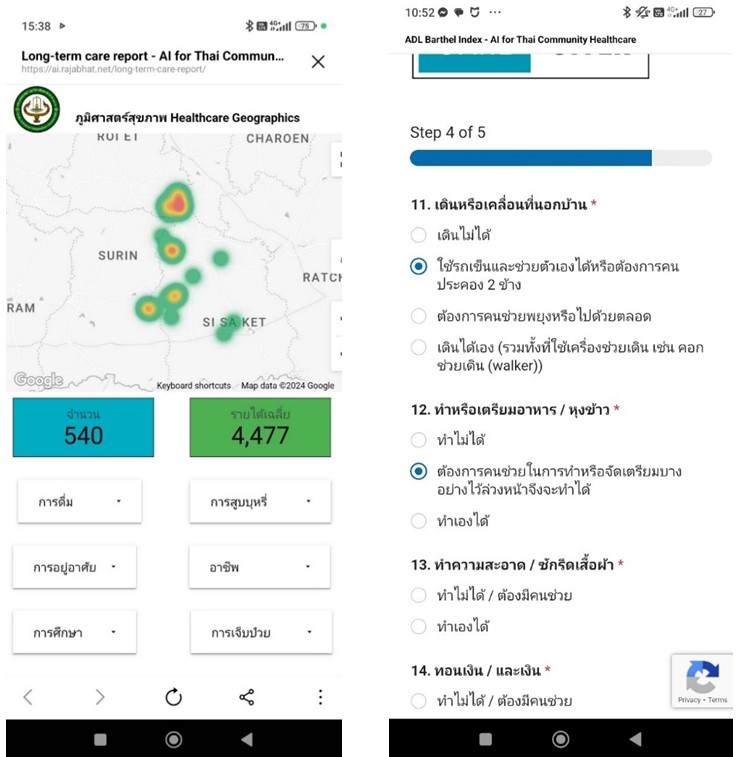
Figure 4: Healthcare Geographics and ADL questionnaire
in "Long-term care" mHealth
To summarize, there is a huge potential in developing an application
for caregivers who are supporting the elderly in long-term care. By
prioritizing user needs, accessibility, and providing comprehensive
support, it creates a valuable tool that can make a real difference in
the lives of both caregivers and the elderly receiving care.
3. Methodology
This study aims to utilize a mobile application for real-time surveys,
such as Activities of Daily Living (ADL) monitoring, stress screening
and others. This leads to earlier detection, improved interventions,
and better health outcomes for individuals in long-term care facilities
compared to traditional methods. By collecting frequent and objective
data on ADL, early detection of functional decline can be achieved.
This is more effective than relying on periodic surveys or
observations. Real-time data insights can enable personalized and
timely interventions to address specific ADL challenges, leading to
improved effectiveness. Therefore, it utilizes a three-phase approach
base on mHealth prototype (Figure 5):
-
Self-Assessment: Users assess their health by using
interactive tools and questionnaires, which helps in developing
datasets.
-
Machine Learning Analysis: Machine learning algorithms
analyze user data to predict health needs and offer personalized
recommendations.
-
Consultant: Users can now easily connect with
healthcare professionals for virtual consultations, improving care
coordination and access to healthcare.
It developed an AI-powered Long-term care app with three phases to
analyze user data and track health progress. The first phase is the
Self-Assessment phase, which provides interactive tools and
questionnaires for users to assess their general health, identify
potential concerns, and track progress. This phase is the beginning of
dataset development. The second phase of the healthcare process involves
the use of machine learning algorithms to analyze user data, such as
their symptoms and health measurements. In this particular mHealth
application, the ADL dataset is collected from local healthcare units.
The dataset is then divided into two separate sets for training and
testing. The accuracy of healthcare predictions is determined by a
confusion matrix, which takes into account several factors including
precision, recall, F1 score, sensitivity, and specificity. Sensitivity
refers to the true positive rate, while specificity refers to the true
negative rate.
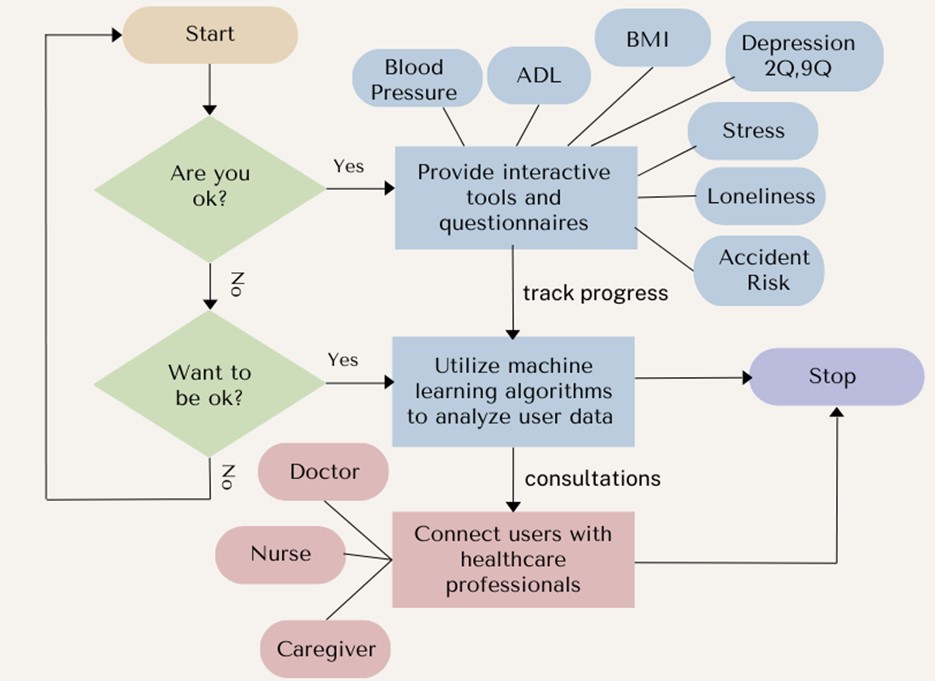
Figure 5: Long-term care mHealth prototype
Table 2: ADL categories
|
ADL
|
ADL Level
|
Focus
|
Activity
|
|
B3
|
Independent Level Score >=12
|
Maintaining independence and promoting
self-management.
|
Encourage individual performance of ADLs like
bathing, dressing, eating,
toileting, and mobility.
|
|
B2
|
Needing Assistance Level
5>=Score <= 11
|
Supporting individuals to safely complete ADLs
while maximizing their participation.
|
Assist with specific tasks or offer modified
approaches (e.g., using adaptive equipment,
providing step-by-step instructions).
|
|
B1
|
Dependent Level 0 >= Score <= 4
|
Ensuring comfort, safety, and dignity while
providing complete care for ADLs.
|
Perform ADLs for the individual, prioritizing
their well-being and addressing specific needs.
|
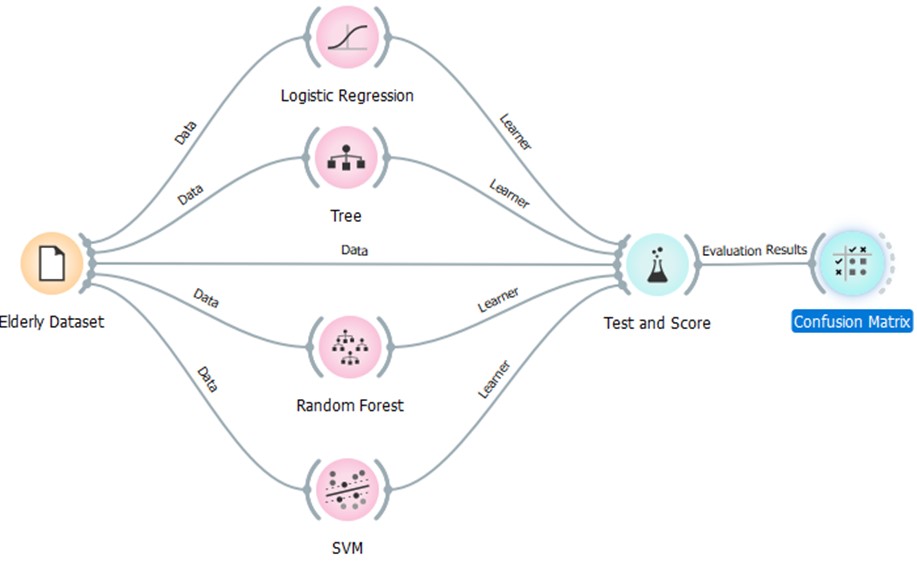
Figure 6: Teaching/Learning the "Long-term care"
mHealth prediction algorithms
The third phase of this study is known as the Consultant phase. In this
phase, users are connected with healthcare professionals, such as
doctors, nurses, or specialists, for virtual consultations through
chat, video calls, or secure messaging. This feature is designed to
help caregivers develop interventions for their community. For the
experiments, we collected a dataset of 913 samples from Ubon
Ratchathani and Sisaket provinces. Descriptive analysis revealed that
the majority of individuals were self-sufficient in their activities of
daily living (ADLs), and a decline in self-sufficiency was observed
with increasing age. Each level of Activities of Daily Living (ADL)
requires different activities to support and take care of an
individual. AI can recommend suitable actions based on an individual's
screening, which can help caregivers reduce their intervention
guidelines by categorizing appropriate activities. This prototype
application analyzes user data to predict healthcare reports for
personal and community sections. Each level of Activities of Daily
Living (ADL) requires different activities to support and take care of
an individual (Table 2). AI can recommend suitable actions based on an
individual's screening, which can help caregivers reduce their
intervention guidelines by categorizing appropriate activities.
3.1 Machine Learning Model Development and Evaluation
To predict healthcare needs and wellness in the elderly population, we
developed a machine learning model using the collected ADL dataset. The
dataset was divided into training and testing sets. Various machine
learning algorithms were explored (Figure 6), including Logistic
Regression, Support Vector Machine (SVM), Random Forest and Trees.
This is a standard machine learning workflow for training and
evaluating various classification algorithms using a dataset related to
the elderly. The Elderly Dataset serves as the initial data source and
contains information about the elderly population, including relevant
features for the target prediction such as ADL scores and demographic
information. The dataset is divided into two subsets (Figure 8):
-
Training Data: This subset is used to train the
machine learning models.
-
Testing Data: Used to evaluate the performance of the
trained models on unseen data.
In this study, we are using different machine learning algorithms to
identify the most suitable model for predicting ADL (Activities of
Daily Living) levels based on the provided samples. Logistic Regression
is a straightforward yet effective algorithm for binary classification
tasks, such as predicting whether an individual is independent or needs
assistance with ADLs. Random Forest and Decision Tree are ensemble
learning methods that combine multiple decision trees to improve
prediction accuracy and robustness. Support Vector Machine (SVM) is a
powerful algorithm for classification and regression tasks and can
handle complex data relationships. The model selection process involved
evaluating each algorithm's performance on the testing set using the
following metrics (Figure 7):
-
Accuracy: The overall proportion of correct
predictions.
-
Precision: The proportion of true positives among
all optimistic predictions.
-
Recall (Sensitivity): The proportion of true
positives among all actual positive instances.
-
F1 Score: A balanced measure combining precision
and recall.
-
Specificity: The proportion of true negatives
among all actual negative instances.
Hyperparameter tuning was performed to optimize each model's
performance. The final model was chosen based on its overall
performance across the selected metrics, with a focus on achieving a
good balance between sensitivity and specificity. The diagram
illustrates the workflow for evaluating and selecting a machine
learning model to predict health outcomes in the elderly population. The
workflow begins with the "Elderly Dataset," which serves as the input
for three different machine learning algorithms: Logistic Regression,
Support Vector Machine (SVM), and Random Forest. Each algorithm is
trained on the dataset using a "Learner" component, which adjusts the
model's parameters to fit the data. The trained models are then
evaluated using a "Test and Score" component, which measures their
performance on a separate portion of the data that wasn't used for
training. This evaluation process involves generating "Predictions" and
comparing them to the actual outcomes, resulting in "Confusion
Matrices" and "Evaluation Results" for each model. The "Confusion
Matrix" provides a detailed breakdown of the model's predictions,
showing the number of true positives, true negatives, false positives,
and false negatives. These values are used to calculate evaluation
metrics like accuracy, precision, recall, and F1-score. The "Evaluation
Results" likely include these performance metrics, as well as other
relevant statistics, helping researchers assess the effectiveness of
each model. The "Tree" component connected to the Random Forest
algorithm suggests that this particular model is based on a decision
tree structure, which can be used to understand how the model makes
predictions.
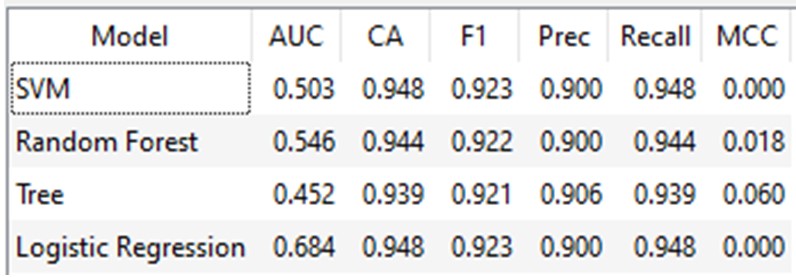
Figure 7: Teaching results for finding the Machine
Learning algorithms
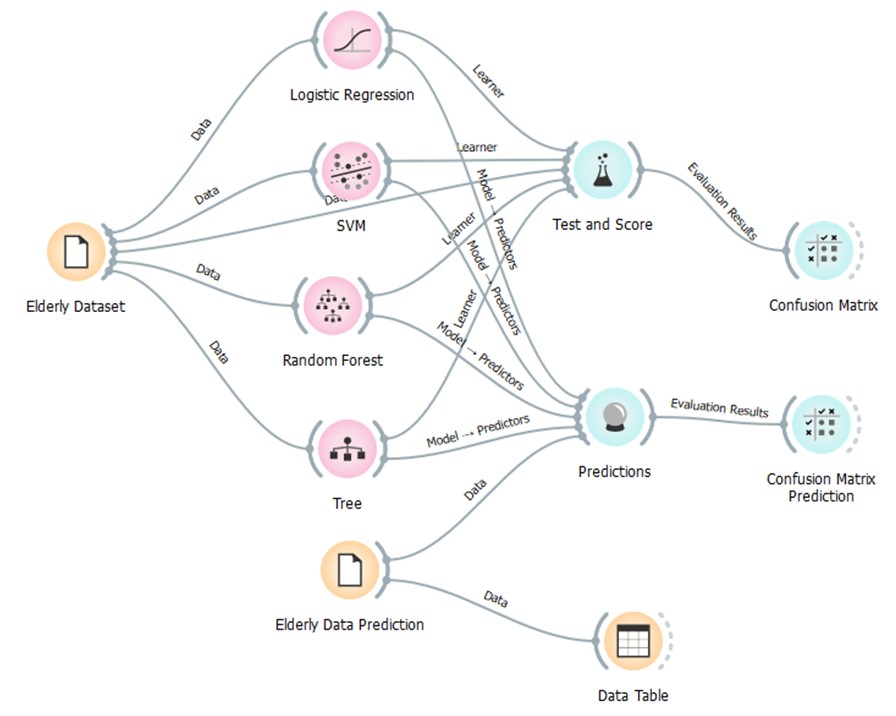
Figure 8: Long-term care mHealth prediction diagram
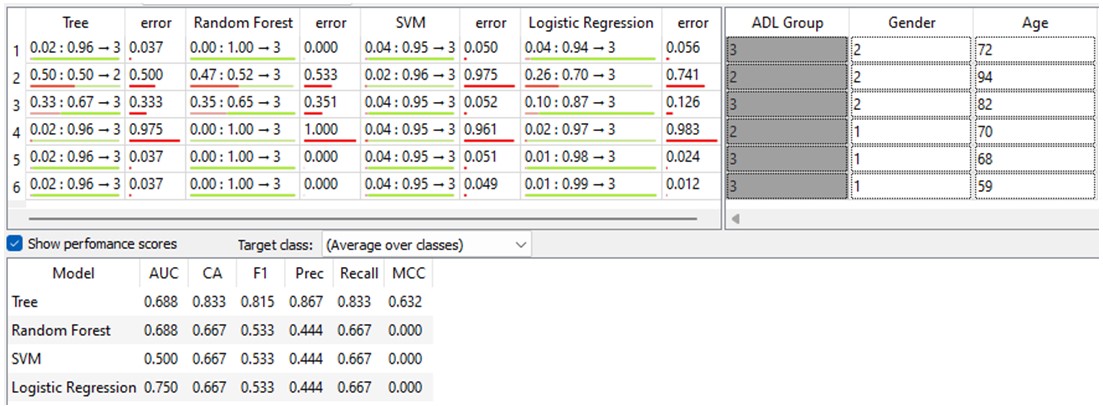
Figure 9: Testing the "Long-term care" mHealth
prediction diagram
Finally, the "Elderly Data Prediction" component appears to represent
the final selected model, which is used to generate predictions for
new, unseen data (Figure 9). These predictions are then stored in a
"Data Table" for further analysis and use in the mHealth application.
In summary, the diagram provides a clear and comprehensive overview of
the machine learning methodology used in the study. It shows how the
researchers explored multiple algorithms, evaluated their performance,
and ultimately chose a model to predict health outcomes in the elderly
population based on their dataset.
AUC (Area Under the Curve): A measure of the model's
ability to distinguish between classes. The Tree and Random Forest
models have the highest AUC (0.688), suggesting better discrimination
than SVM (0.500). Logistic Regression has the best AUC (0.750) among
all the models.
-
CA (Classification Accuracy): The proportion of
correct predictions. The Tree model outperforms the others with the
highest CA (0.833).
-
F1 Score: A balanced measure of precision and recall.
The Tree model again excels with the highest F1 score (0.815).
-
Precision: The proportion of true positives among
predicted positives. The Tree model demonstrates the best precision
(0.867).
-
Recall: The proportion of true positives among actual
positives. All models except the Tree model have a recall of 0.667.
-
MCC (Matthews Correlation Coefficient): A measure of
the quality of binary classifications. The Tree model has the highest
MCC (0.632), indicating the best overall performance.
Therefore, the Tree model demonstrates superior performance in
predicting ADL group membership compared to Random Forest, SVM, and
Logistic Regression, as evidenced by its higher AUC, CA, F1 score,
precision, and MCC. However, Logistic Regression exhibits the best
discrimination of classes based on its AUC value. These findings
suggest that the Tree model may be the most suitable for predicting ADL
levels in this specific context, although further analysis and
validation might be necessary to confirm its generalizability. This
application uses user data to predict the healthcare needs of the
elderly population and facilitate support from local healthcare units.
This dataset contains 913 samples collected from Ubon Ratcha Thani and
Sisaket provinces in Thailand. The Likert-type scale for ADL items
ranges from 1 (Unable) to 4 (Independent) in Table 3. The dataset was
used for descriptive analysis, principal component analysis, and
machine learning model development.
Table 3: Elderly dataset description
|
Feature
|
Description
|
Data Type
|
Measurement Scale
|
|
Range/Values
|
|
Age
|
Participant's age in years
|
Numerical (Integer)
|
Ratio
|
|
19-98
|
|
ADL Level
|
Assessment of Activities of Daily Living (ADL)
|
Categorical
|
Ordinal
|
|
B1 (Dependent), B2 (Needing Assistance), B3
(Independent)
|
|
Feeding
|
Ability to feed oneself
|
Ordinal
|
Likert-type
(1-4)
|
|
1 (Unable), 4 (Independent)
|
|
Grooming
|
Ability to maintain personal hygiene (e.g.,
brushing teeth, combing hair)
|
Ordinal
|
Likert-type
(1-4)
|
|
1 (Unable), 4 (Independent)
|
|
Transfer
|
Ability to move from one position to another
(e.g., bed to chair)
|
Ordinal
|
Likert-type
(1-4)
|
|
1 (Unable), 4 (Independent)
|
|
Toilet Use
|
Ability to use the toilet independently
|
Ordinal
|
Likert-type
(1-4)
|
|
1 (Unable), 4 (Independent)
|
|
Mobility
|
Ability to walk and move around
|
Ordinal
|
Likert-type
(1-4)
|
|
1 (Unable), 4 (Independent)
|
|
Dressing
|
Ability to dress oneself
|
Ordinal
|
Likert-type
(1-4)
|
|
1 (Unable), 4 (Independent)
|
|
Stairs
|
Ability to climb stairs
|
Ordinal
|
Likert-type
(1-4)
|
|
1 (Unable), 4 (Independent)
|
|
Bathing
|
Ability to bathe oneself
|
Ordinal
|
Likert-type
(1-4)
|
|
1 (Unable), 4 (Independent)
|
|
Bowels
|
Ability to control bowel movements
|
Ordinal
|
Likert-type
(1-4)
|
|
1 (Unable), 4 (Independent)
|
|
Bladder
|
Ability to control bladder function
|
Ordinal
|
Likert-type
(1-4)
|
|
1 (Unable), 4 (Independent)
|
|
Others
|
(Additional features may include stress,
loneliness scales, and other health-related
measurements)
|
Varies
|
Varies
|
|
Varies
|
4. Experiments and Design Results
The focus of this study is to use mobility services to aid caregivers
and the local community in accessing healthcare services. To achieve
this goal, there is a need for tools that can improve the provision of
services and support from the local government. Moreover, if these
tools can predict or estimate the impact of elderly individuals on
healthcare services, it can help the healthcare center plan for the
necessary intervention protocols, considering the number of caregivers
available to support the community. Descriptive analysis results from
913 samples of 3 districts and 4 sub-districts in Ubon Ratch Thani and
Sisaket provinces. This report provides a summary of the descriptive
analysis of the relationship between age and ADL (Activities of Daily
Living) levels present in the data in Table 4. The findings indicate
that most individuals (94.74%) belonged to age group B3, representing
an independent level of ADL. The remaining individuals were distributed
in age groups B2 (3.83%), which means a need for assistance, and B1
(1.42%), which represents a dependent level. Additionally, the average
age for all groups was 69.95 years old, ranging from 19 to 98 years
old.
As per the Age and ADL Level analysis, there was a noticeable pattern
of declining independence with advancing age. Individuals in the
independent group (B3) were generally younger than those in the group
needing assistance (B2) and the dependent group (B1). The group needing
help (B2) had the highest standard deviation, indicating more
significant age variability within this group than the others. This
analysis provides a basic understanding of how age and ADL levels are
related. Further investigation is needed to draw more definitive
conclusions and identify potential factors influencing ADL performance
as a histogram. The histogram (Figure 10) shows a skewed distribution
towards the older age groups, which is consistent with the following:
X-axis: Age groups ranging from 20-24 to 80-84 years.
Y-axis: Probability, likely ranging from 0 to 0.2 (20%).
For the AI data-driven, the additional questions that could be explored
such as what factors besides age might influence an individual's ADL
level.
Table 4: Descriptive analysis of ADL by age
|
Frequency
|
%
|
Mean
|
Std. Deviation
|
Variance
|
Minimum
|
Maximum
|
|
Age
|
B3
|
865
|
94.74%
|
69.99
|
8.22
|
67.57
|
19
|
96
|
|
B2
|
35
|
3.83%
|
77.6
|
11.32
|
128.25
|
56
|
113
|
|
B1
|
13
|
1.42%
|
75.38
|
10.92
|
119.26
|
58
|
98
|
B3: Independent Level B2: Needing Assistance Level B1: Dependent
Level
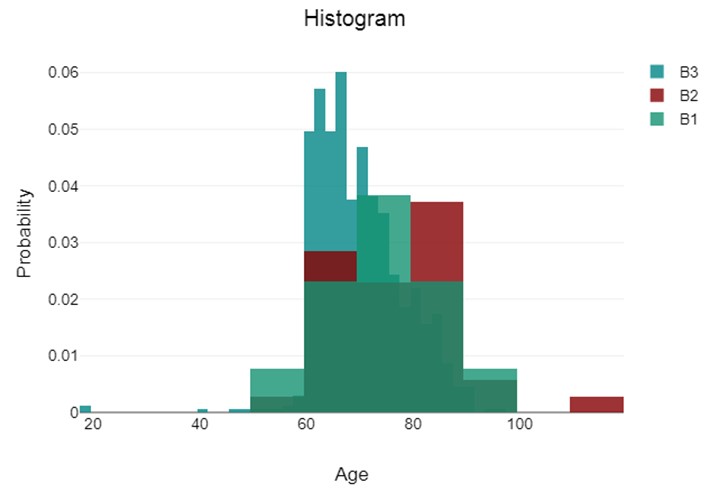
Figure 10: ADL histogram probability and age
This study aims to gain deeper insights into the relationship between
age and Activities of Daily Living (ADL) performance by addressing
certain questions and considering potential limitations. The study
utilizes Principal Component Analysis (PCA) with Varimax rotation on a
dataset assessing ADL performance to identify underlying factors that
explain the interrelationships between different ADLs. The results of
this study will be used to develop features for an AI model that
predicts wellness in the local community.
This Table 5 presents a correlation matrix summarizing the
relationships between ten activities of daily living (ADLs): feeding,
grooming, transferring, toilet use, mobility, dressing, stairs,
bathing, bowels, and bladder. The values in the table represent the
correlation coefficients between each pair of ADLs, ranging from -1
(perfect negative correlation) to +1 (perfect positive correlation).
Most correlations are positive, indicating that individuals who perform
well in one ADL tend to also perform well in others. The strength of
these correlations varies, with some activities exhibiting stronger
relationships than others. Transferring, toilet use, mobility, and
dressing show the strongest positive correlations (coefficients above
0.75), suggesting they share a common underlying factor related to
physical movement and independence.
Grooming, bathing, and dressing also have relatively strong
correlations (around 0.65), potentially reflecting shared aspects of
self-care and personal hygiene. The components represent these
underlying factors, and the percentages in the "Total % of Variance"
column indicate their relative importance in explaining the overall
variations observed in the ADL data in Table 6.
Table 5: Correlation matrix
|
Feature
|
Feeding
|
Grooming
|
Transfer
|
Toilet use
|
Mobility
|
Dressing
|
Stairs
|
Bathing
|
Bowels
|
Bladder
|
|
Feeding
|
1
|
0.57
|
0.69
|
0.62
|
0.68
|
0.65
|
0.62
|
0.54
|
0.41
|
0.41
|
|
|
Grooming
|
0.57
|
1
|
0.66
|
0.62
|
0.66
|
0.68
|
0.53
|
0.66
|
0.39
|
0.37
|
|
|
Transfer
|
0.69
|
0.66
|
1
|
0.79
|
0.84
|
0.79
|
0.72
|
0.64
|
0.52
|
0.52
|
|
|
Toilet use
|
0.62
|
0.62
|
0.79
|
1
|
0.81
|
0.82
|
0.76
|
0.72
|
0.52
|
0.49
|
|
|
Mobility
|
0.68
|
0.66
|
0.84
|
0.81
|
1
|
0.79
|
0.75
|
0.68
|
0.53
|
0.48
|
|
|
Dressing
|
0.65
|
0.68
|
0.79
|
0.82
|
0.79
|
1
|
0.77
|
0.75
|
0.55
|
0.55
|
|
|
Stairs
|
0.62
|
0.53
|
0.72
|
0.76
|
0.75
|
0.77
|
1
|
0.59
|
0.53
|
0.52
|
|
|
Bathing
|
0.54
|
0.66
|
0.64
|
0.72
|
0.68
|
0.75
|
0.59
|
1
|
0.4
|
0.43
|
|
|
Bowels
|
0.41
|
0.39
|
0.52
|
0.52
|
0.53
|
0.55
|
0.53
|
0.4
|
1
|
0.77
|
|
|
Bladder
|
0.41
|
0.37
|
0.52
|
0.49
|
0.48
|
0.55
|
0.52
|
0.43
|
0.77
|
1
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Table 6: Total of variance
|
Component
|
Total
|
Variance (%)
|
Accumulated (%)
|
|
1
|
6.63
|
66.27
|
66.27
|
|
2
|
1.05
|
10.45
|
76.72
|
|
3
|
0.53
|
5.29
|
82.01
|
|
4
|
0.46
|
4.59
|
86.6
|
|
5
|
0.34
|
3.39
|
89.99
|
|
6
|
0.28
|
2.76
|
92.75
|
|
7
|
0.23
|
2.33
|
95.08
|
|
8
|
0.19
|
1.88
|
96.96
|
|
9
|
0.17
|
1.66
|
98.62
|
|
10
|
0.14
|
1.38
|
100.00
|
Additionally, the first component explains the largest portion of the
variance (6.63%), suggesting it captures the most significant
underlying factor influencing ADLs in this dataset. The remaining
components contribute progressively smaller portions of variance,
implying they represent less prominent but potentially still relevant
factors. By the 10th component, the accumulated explained variance
reaches 100%, indicating that all the relevant information from the
original data is captured by these ten components. This table shows
three components that help to classify different activities of daily
living (ADLs) based on their importance for physical independence and
functional ability (Table 7). Component 1 has high positive loadings
(above 0.7) for most basic ADLs, such as feeding, grooming, transfer,
toilet use, mobility, dressing, stairs, and bathing. This suggests that
it captures a general factor related to overall physical independence
and functional ability for basic ADLs. On the other hand, component 2
shows moderate positive loadings for bathing (0.38) and grooming (0.4),
along with a negative loading for bowels (-0.65). This might indicate a
factor associated with personal care and hygiene, potentially influenced
by dexterity and upper body movement to some extent.
Finally, component 3 has high positive loadings for both bowels (0.68)
and bladder (0.66), suggesting it isolates a distinct factor
specifically related to elimination functions. In summary, these
components help to understand the importance of different ADLs for
physical independence and functional ability, as well as the factors
that influence personal care and hygiene and elimination functions.
Finally, the results obtained from Varimax are presented as follows
(Table 8):
Component 1: Overall Physical Independence (0.61 - 0.78)
This component has high positive loadings for most ADLs (feeding,
transfer, toilet use, mobility, dressing, stairs), suggesting it
captures a general factor related to overall physical independence and
functional ability for basic ADLs.
Component 2: Elimination Functions (0.8 - 0.91)
This component demonstrates high positive loadings for both bowels and
bladder, indicating that it isolates a distinct factor that is
specifically related to the management of urinary and bowel functions.
Component 3: Personal Care and Hygiene (0.8 - 0.82)
This component has high positive loadings for grooming and bathing,
suggesting it represents a factor associated with self-care and
personal hygiene, potentially involving aspects of upper body movement
and coordination.
Table 7: Component matrix
|
Feature
|
Components
|
|
1
|
2
|
3
|
|
1. Feeding
|
0.77
|
-0.16
|
-0.32
|
|
2. Grooming
|
0.76
|
-0.26
|
0.4
|
|
3. Transfer
|
0.89
|
-0.1
|
-0.13
|
|
4. Toilet use
|
0.89
|
-0.12
|
-0.06
|
|
5. Mobility
|
0.9
|
-0.13
|
-0.11
|
|
6. Dressing
|
0.91
|
-0.07
|
0.04
|
|
7. Stairs
|
0.84
|
0
|
-0.28
|
|
8. Bathing
|
0.79
|
-0.22
|
0.38
|
|
9. Bowels
|
0.68
|
0.65
|
0.05
|
|
10.Bladder
|
0.66
|
0.66
|
0.1
|
Table 8: Rotated Component Matrix (Varimax)
|
Feature
|
Components
|
|
1
|
2
|
3
|
|
1. Feeding
|
0.78
|
0.2
|
0.25
|
|
2. Grooming
|
0.32
|
0.18
|
0.82
|
|
3. Transfer
|
0.72
|
0.34
|
0.43
|
|
4. Toilet use
|
0.68
|
0.33
|
0.5
|
|
5. Mobility
|
0.72
|
0.32
|
0.47
|
|
6. Dressing
|
0.61
|
0.39
|
0.56
|
|
7. Stairs
|
0.76
|
0.39
|
0.26
|
|
8. Bathing
|
0.35
|
0.24
|
0.8
|
|
9. Bowels
|
0.22
|
0.9
|
0.16
|
|
10. Bladder
|
0.17
|
0.91
|
0.19
|
5. Conclusion and Future Works
This study has successfully developed mobile health technology
(mHealth) that utilizes principal component analysis (PCA) as a
data-driven approach. However, to design effective and ethical
intervention protocols for caregivers who support older adults in their
activities of daily living (ADL) needs, it is essential to combine the
insights obtained from PCA with clinical expertise and individual
considerations. It highlights that while mHealth can be a useful tool
that cannot replace the human touch, empathy, and judgment of a
caregiver. The study's success lies in the mHealth application that
uses the LINE platform to bridge the gap between caregivers and local
healthcare units in the community. This application establishes a
direct connection with participants, making it convenient for the
government and community to track and monitor community wellness. It is
important to note that recommendations such as healthcare promotion or
intervention protocol should be evaluated and adapted carefully based
on the individual's unique situation.
In future works, the identified features will be used to determine
suitable services for interventions aimed at improving the well-being
of the local community. The insights gained from analyzing the ADL
dataset using techniques like PCA can provide valuable information for
developing targeted and comprehensive interventions to enhance the
well-being of the local community. By addressing the various factors
that affect ADLs and adopting a holistic approach, communities can
create a supportive environment that promotes independence, dignity,
and overall well-being for their residents.
Acknowledgment
We deeply appreciate the support from each of these organizations.
Their contributions were instrumental to the success of this research
endeavor. Bureau of Public Health Research and Innovation
Administration, Division of Academic Affairs, Department of General
Secretary, Ministry of Public Health for providing essential funding
that made this research possible. Tropical Health
Innovation Research Unit, Faculty of Medicine, Mahasarakham University
for generously offering facilities that enabled our research
work. Valaya Alongkorn Rajabhat University under the
Royal Patronage for providing the valuable dataset crucial to our
analysis in this study. The Faculty of Medicine, Mahasarakham
University, a leading institution in medical education and research in
Thailand, has supported this research. The faculty and staff are
grateful for the opportunity to have worked with such a talented and
dedicated team.
[1] Czaja, S. J., (2016). Long-term Care Services and Support Systems
for Older Adults: The Role of Technology. Am Psychol, Vol. 71(4).
294–301.
https://doi.org/10.1037/a0040258.
[2] Sato, J., Mitsutake, N., Kitsuregawa, M., Ishikawa, T. and Goda, K.,
(2022). Predicting Demand for Long-Term Care Using Japanese Healthcare
Insurance Claims Data. Environ Health Prev Med, Vol. 27(1).
https://doi.org/10.1265/ehpm.22-00084.
[3] Sin, J., Henderson, C., Spain, D., Cornelius, V., Chen. T. and
Gillard, S., (2018). eHealth Interventions for Family Carers of People with
Long Term Illness: A Promising Approach?. Clin Psychol Rev, Vol.
60, 109–125.
https://doi.org/10.1016/j.cpr.2018.01.008.
[4] Wieczorek, E., Kocot, E., Evers, S., Sowada, C. and Pavlova, M.,
(2023). Development of a Tool for Assessing the Performance of Long-Term
Care Systems in Relation to Care Transition: Transitional Care Assessment
Tool in Long-Term Care (TCAT-LTC). BMC Geriatr, Vol. 23(1).
https://doi.org/10.1186%2Fs12877-023-04467-z.
[5] Tabi, K., Randhawa, A. S., Choi, F., Mithani, Z., Albers, F.,
Schnieder, M., Nikoo, M., Vigo, D., Jang, K., Demlova, R. and Krausz, M.,
(2019). Mobile Apps for Medication Management: Review and Analysis,
JMIR Mhealth Uhealth
, Vol. 7(9).
https://doi.org/10.2196/13608.
[6] Lugones-Sanchez, C., Recio-Rodriguez, J. I., Agudo-Conde, C.,
Repiso-Gento, I. G., Adalia E, Ramirez-Manent, J. I., Sanchez-Calavera, M.
A., Rodriguez-Sanchez, E., Gomez-Marcos, M. A. and Garcia-Ortiz, L.,
(2022). Long-term Effectiveness of a Smartphone App Combined with a Smart
Band on Weight Loss, Physical Activity, and Caloric Intake in a Population
with Overweight and Obesity (Evident 3 Study): Randomized Controlled Trial.
J Med Internet Res, Vol. 24(2).
https://doi.org/10.2196/30416.
[7] Penkunas, M. J., Eom, K. Y. and Chan, A. W., (2017). Classification
Trees for Identifying Non-Use of Community-Based Long-Term Care Services
among Older Adults. Health Policy, Vol. 121(10). 1093–1099.
https://doi.org/10.1016/J.HEALTHPOL.2017.05.008.
[8] Samoggia, A. and Riedel, B., (2020). Assessment of Nutrition-Focused
Mobile Apps’ Influence on Consumers’ Healthy Food Behaviour and Nutrition
Knowledge. Food Res Int, Vol. 128.
https://doi.org/10.1016/J.FOODRES.2019.108766.
[9] Cui, X., Zheng, X. and Lu, Y., (2024). Prediction Model for
Cognitive Impairment among Disabled Older Adults: A Development and
Validation Study. Healthcare (Switzerland), Vol. 12(10).
https://doi.org/10.3390/healthcare12101028.
[10] Pavon, J. M., Previll, L., Woo, M., Henao, R., Solomon, M., Rogers,
U., Olson, A., Fischer, J., Leo, C., Fillenbaum, G., Hoenig, H. and
Casarett, D., (2023). Machine Learning Functional Impairment Classification
with Electronic Health Record Data. J Am Geriatr Soc., Vol. 71(9).
2822–2833.
https://doi.org/10.1111/JGS.18383.
[11] Li, Q., Zhao, Y., Chen, Y., Yue, J. and Xiong, Y., (2022). Developing
a Machine Learning Model to Identify Delirium Risk in Geriatric Internal
Medicine Inpatients. Eur Geriatr Med, Vol. 13(1). 173–183.
https://doi.org/10.1007/S41999-021-00562-9.
[12] Lin, S., Wu, Y. and Fang, Y., (2022). A Hybrid Machine Learning Model
of Depression Estimation in Home-Based Older Adults: A 7-year Follow-Up
Study. BMC Psychiatry, Vol. 22(1).
https://doi.org/10.1186/S12888-022-04439-4.
[13] Perez, H., Miguel-Cruz, A., Daum, C., Comeau, A. K., Rutledge, E.,
King, S. and Liu, L., (2022). Technology Acceptance of a Mobile Application
to Support Family Caregivers in a Long-Term Care Facility.
Appl Clin Inform
, Vol. 13(5), 1181–1193.
https://doi.org/10.1055/A-1962-5583.
[14] Paul, M., Maglaras, L., Ferrag, M. A. and Almomani, I., (2023).
Digitization of Healthcare Sector: A Study on Privacy and Security
Concerns. ICT Express, Vol. 9(4), 571–588.
https://doi.org/10.1016/J.ICTE.2023.02.007.
[15] Chen, M. C., Kao, C. W., Chiu, Y. L., Lin, T. Y., Tsai, Y. T., Jian,
Y. Z., Tzeng, Y. M., Lin, F. G., Hwang, S. L., Li, S. R. and Kao, S.,
(2017). Effects of Home-Based Long-Term Care Services on Caregiver Health
According to Age. Health Qual Life Outcomes, Vol. 15(1).
https://doi.org/10.1186/S12955-017-0786-6.
[16] Robič, M. and Pavlič, D. R., (2021). COVID-19 and Care for the
Elderly in Long-Term Care Facilities: The Role of Information Communication
Technology. Acta Med Acad, Vol. 50(3), 414–422.
https://doi.org/10.5644/AMA2006-124.363.
[17] Knodel, J., Teerawichitchainan, B. and Pothisiri, W., (2018). Caring
for Thai Older Persons with Long-Term Care Needs. J Aging Health,
Vol. 30(10), 1516–1535.
https://doi.org/10.1177/0898264318798205.
[18] Lee, E. Y., Cha, S. A., Yun, J. S., Lim, S. Y., Lee, J. H., Ahn, Y.
B., Yoon, K. H., Hyun, M. K. and Ko, S. H., (2022). Efficacy of
Personalized Diabetes Self-care Using an Electronic Medical
Record-Integrated Mobile App in Patients with Type 2 Diabetes: 6-Month
Randomized Controlled Trial. J Med Internet Res., Vol. 24(7).
https://doi.org/10.2196/37430.
[19] Wayan Pulantara, I., Parmanto, B. and Germain, A., (2018).
Development of a Just-in-Time Adaptive mHealth Intervention for Insomnia:
Usability Study. JMIR Hum Factors, Vol. 5(2).
https://doi.org/10.2196/HUMANFACTORS.8905.
[20] Nadal, C., Sas, C. and Doherty, G., (2020). Technology Acceptance in
Mobile Health: Scoping Review of Definitions, Models, and Measurement.
J Med Internet Res, Vol. 22(7).
https://doi.org/10.2196/17256.
